Weighting factors based on observed RCA, LCX and LAD anatomy
Based on the standard 17 segment model of the LV, the weighting factors are derived from the above-described anatomic details of RCA, LAD, LCX or their branches (variations in coronary anatomy). The benchmark pattern of coronary circulation is used as reference and weighting factors with discrete values are added to account for the variations in circulation pattern. Use of preset, discrete incremental values is a compromise between the convenience of clinical use and the variability in coronary artery circulation. A preset incremental value of 1 or 1.5 was used to describe differences in in LAD length, in diagonal branch size or in RCA supply territory as listed in tables 3, 4 and 5.
Table 3. Progressive LAD weighting factor changes (with a step size of 1.0) across LAD lengths with both the same RCA dominance (for example, average) and the same diagonal size (for example, small).
RCA | Average RCA dominant | |||
Dx | Small | |||
LAD | Short | Ave. | Long | |
seg 5 | LM | 11 | 12 | 13 |
seg 6 | Prox. LAD | 4.5 | 5.5 | 6.5 |
seg 7& | Mid LAD& | 3.5 | 4.5 | 5.5 |
seg 7X | Mid LADx | 3 | 4 | 5 |
seg 7S | Mid LADs | 2.5 | 3.5 | 4.5 |
seg 7E | Mid LADe | 2.75 | 3.75 | 4.75 |
seg 7 | Mid LAD | 2 | 3 | 4 |
seg 8 | Distal LAD | 1 | 2 | 3 |
Notes: Abbreviations as listed in table 2.
Table 4. Progressive diagonal weighting factor changes (with a step size of 1.5) across diagonal sizes with both the same LAD length (for example, short) and the same RCA dominance (for example, small).
RCA | Small RCA dominant | |||
Dx | Small | Inter. | Large | |
LAD | Short | |||
seg 9& | Comb. Dx | 1.5 | 3 | 4.5 |
Notes: Abbreviations as listed in table 2.
Table 5. Progressive RCA weighting factor changes (with a step size of 1.5) across RCA dominances with both the same diagonal size (for example, intermediate) and the same LAD length (for example, average).
| RCA | PDA zero | PDA only | Small RCA | Average RCA | Large RCA | Super RCA | |
Dx | Inter. | Inter. | Inter. | Inter. | Inter. | Inter. | ||
LAD | Ave. | Ave. | Ave. | Ave. | Ave. | Ave. | ||
RCA | seg 1 | Prox. RCA | NULL | 2 | 3.5 | 5 | 6.5 | 8 |
Notes: Abbreviations as listed in table 2.
Weighting factor assignment for coronary artery tree segments in different RCA dominances with different LAD lengths or diagonal sizes
Weighting factors for coronary artery tree segments in the benchmark type are shown as reference, and a preset segment number difference of 1.0 or 1.5 is highlighted in golden. This approach allows to derive the weighting factors for all the coronary artery tree segments in the 54 types of coronary artery circulation proposed in this angiographic scoring system (table 6).
--Weighting factor derivation for PDA and PLVs
The septal wall (anterior and inferior) with 6 segments according to the benchmark type is perfused competitively by LADex and PDA. Therefore, their weighting factor sum is always 6.0 regardless of LAD lengths. Understandably, weighting factor for segment 4 (PDA) is 3.0, 2.0 and 1.0, respectively, corresponding to short, average and long LAD length, respectively.
The inferior wall with 3 segments according to the benchmark type is perfused competitively by PLVs arising from RCA or LCX. Therefore, their weighting factor sum is always 3.0 regardless of RCA dominances. Understandably, weighting factor for segment 14& is constantly 3.0 in PDA zero or PDA only; the weighting factor for segment 16& is constantly 3.0 in average, large or super RCA dominant; and the weighting factor sum of segments 14& and 16& is constantly 3.0 in Small RCA dominant. Segment 16c represents obtuse marginal arteries arising from segment 16 and its weighting factor is 1.5 and 3.0 in large and super RCA dominant, respectively. Thus, the weighting factors for segment 1, 2 or 3 equal the weighting factor sum of segments 4 and 16 in the corresponding cells. The weighting factors for segment 16 equals the weighting factor sum of segments 16& and 16c in the corresponding cells.
--Weighting factor derivation for Dx and LAD
Referring to the benchmark type, weighting factors for Dx (segment 9&) are 2.0, 3.0 and 4.0, respectively, according to different sizes of Dx. Weighting factors for LAD segments depend both on the segment numbers they supply and on the diagonals arising as shown in Figure 10.

Figure 10. Weighting factor derivation for LAD segments. Suppose an average LAD length with a Dx take-off. Segment 8 of LAD provides blood supply to the apical anterior septum and apex segment with 2 segments; thus, the weighting factor for segment 8 is 2.0. Segment 7 provides blood supply to the mid anterior septum, apical anterior septum and apex segment with 3 segments; thus, the weighting factor for segment 7 is 3.0. Likewise, the weighting factor for segment 6 is 4.0 in the absence of a Dx. As a matter of fact, segment 6 gives rise to a Dx; therefore, its weighting factor should incorporate the contribution by the Dx. Suppose the weighting factor for the Dx is 1.5 and the weighting factor for segment 6 should therefore be 5.5.
--Weighting factor derivation for LCX and obtuse marginal arteries
The weighting factors for the LCX are indirectly derived from the weighting factor differences between LM and LAD in the corresponding cells, briefly expressed as LCX=LM-LAD or Seg 11=Seg 5–Seg 6). The weighting factors for segment 12& are indirectly derived from the weighting factor differences between segments 11 and 13 in the corresponding cells (Seg 12&=Seg 11-Seg 13).
Table 6. Weighting factors assigned to coronary artery tree segments in different RCA dominances with different sizes of diagonals or lengths of LAD.

Notes: the benchmark pattern of coronary circulation is used as reference and weighting factors with discrete values in the golden cells are added to account for the variations in circulation pattern. Values assigned in the green cells strictly obey the matrix operations. Values assigned in the yellow cells are fractions of those marked with &’, among which values marked with X’ or S’ with a difference of 0.5. RCA=right coronary artery; LAD=left anterior descending; LCX=left circumflex; OM=obtuse marginal; Dx=diagonals; Comb. Dx=all the diagonals arising from LAD; PDA=posterior descending artery; and Comb. PLVs=all the posterolateral vessels arising from LCX or RCA.
Lesion scoring and the need for adapting modfications
The degree of stenosis is also considered in deriving the lesion scoring. If the blood vessel is totally occluded, the coronary artery segment weighting value is multiplied by 5.0. If the blood vessel is more than 50-99% diameter stenosis, the value is multiplied by 2.0. The lesion score is a product of the weighting factor of a blood vessel and its stenosis degree. The coronary artery lesion scores will then be added to derive the total score(15). A score of zero indicates no stenosis of coronary artery tree, and the higher the score, the greater the stenosis is. Within one segment, direct scoring will overestimate the severity of coronary artery disease in the presence of significant side branches (SB, >1.5 mm in diameter) preceding the main branch (MB) lesion regardless of their normal or diseased status. Thus, lesion scoring should be modified as shown in Figure 11.
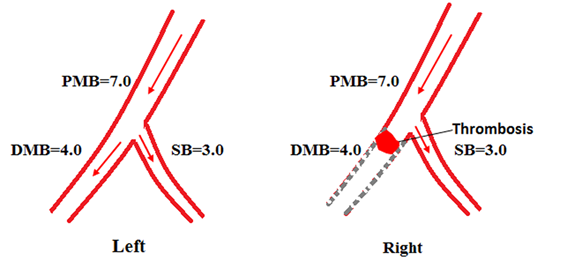
Figure 11. Lesion scoring modification within one segment in the presence of a significant branch (SB). Arrow=blood flow direction; PMB=proximal main branches; DMB=distal main branches; SB=side branch; dashed gray lines=occluded segment distal to the occlusive lesion. We often encounter a coronary artery segment with a take-off of a significant side branch (SB). Suppose the weighting factor is 7.0 for this segment and 3.0 for the SB. The main branch (MB) of the segment divides into proximal or distal MB referring to the SB. According to the law of flow conservation, the weighting factor for the distal MB is 4.0 (Left). Within one segment, an occlusive lesion for this segment distal to the SB (DMB lesion) is scored as 7.0×5=35.0 according to the CatLet scoring algorithm (Right). Actually, the DMB lesion’s weighting factor is only 4.0 because of the presence of the SB. Hence, the CatLet scoring algorithm overestimates the severity of the occlusive DMB lesion. The scoring values for this segment should be modified for 7.0×5-3.0×5=20.0 using formula 1.
The scoring modification is required in the following 6 scenarios according to corresponding formulas.
Occluded lesions
In case of an occluded MB lesion preceded by an intact significant SB in a segment (1 lesion) (Figure 12a), the final score for the lesion should be modified via Formula 1 as the weighting factor of the MB has covered the intact SBs’, which is actually not adversely affected.
S=subtotal score -W SBs×5; (1)
In case of an occluded MB lesion preceded by an involved significant SB in a segment (within 1 lesion) (Figure 12b), the final score for the lesion is modified via Formula 2 as the MB and the SB will be scored simultaneously as one lesion. As a matter of fact, the weighting factor of the MB has already covered the SB’s.
S=subtotal score-W SBs×8 (2)
In case of an occluded MB lesion preceded by a separate lesion on SBs (2 separate lesions, one is on the MB and the other is on the SB) in a segment (Figure 12c), final score for the MB lesion is modified via Formula 3 as the weighting factor of the MB lesion covered the diseased SBs’, which should be subtracted from that of the MB. The lesion on the SB will be scored separately.
S = subtotal score-W SBs×5; (3)
Non-occluded lesions
In case of a non-occluded MB lesion preceded by intact SBs in a segment (1 lesion) (Figure 12d), the final score for the MB lesion is modified via Formula 4 as the weighting factor of the MB lesion has covered the intact SBs’, which is actually not adversely affected.
S =subtotal score-W SBs×2; (4)
In case of a non-occluded MB lesion preceded by an involved significant SB in a segment (within 1 lesion) (Figure 12e), the final score for the lesion is modified via formula 5 as the MB and the SBs will be scored simultaneously as one lesion, in which the weighting factor of the MB has already covered the SBs’.
S=subtotal score-W SBs×2; (5)
In case of a non-occluded MB lesion preceded by a separate lesion on SBs (2 separate lesions) in a segment (Figure 12f), the final score for the MB lesion is modified via Formula 6 as the weighting factor of the MB lesion has already covered the SBs’, which should be subtracted from the MB’s. The lesion on the SBs will be scored separately.
S= subtotal score - W SBs×2; (6)
Where S is the modified score for a lesion;
W is the weighting factor of side branches;
Subtotal score is calculated for the lesion according to the CatLet scoring algorithm.
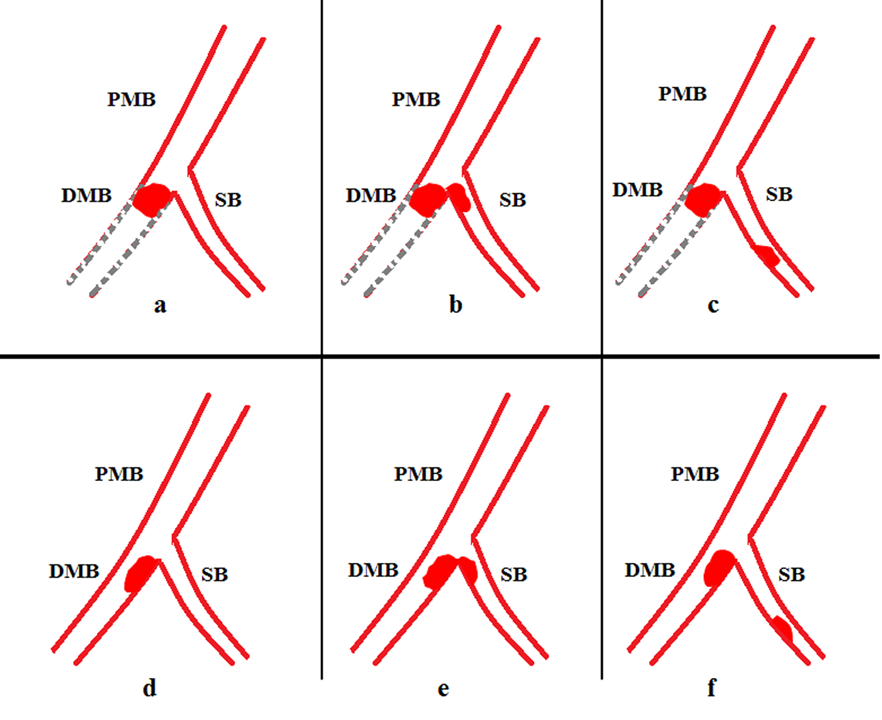
Figure 12. Lesion scoring modification within one segment in the 6 circumstances. The upper row is for the occluded lesion and the lower row is for the non-occluded lesion. PMB or DMB indicates proximal or distal major branches and SB indicates side branches. Dashed gray lines indicate occluded blood vessels distal to the occluded lesion. Figures a & d indicated 1 lesion involving the DMB; Figures b & e indicate 1 lesion involving both the DMB and the SB; and Figures c & f indicate 2 separate lesions involving the DMB and the SB.
发表评论:
◎Welcome to participate in the discussion, please post your views here and exchange your views.