Derivation of a 17 myocardial segmentation-based (CatLet) angiographic scoring system and its algorithm
By Yong-Ming He, MD, PhD, Ming-Xing Xu, MD
Division of Cardiology, The First Affiliated Hospital of Soochow University
E-mail: heyongming@catletscore.com or heyongming@suda.edu.cn
Give me a reference and a ruler, and I can characterize all the variations of coronary anatomy.
Identity and difference make a world.
------By Matthew Yong-Ming He
It is strongly recommended that you should read through the SYNTAX score before you start this
tutorial.(https://www.ncbi.nlm.nih.gov/pubmed/19758907)
The CatLet score in PDF version is available now at http://jtd.amegroups.com/article/view/34094 & https://onlinelibrary.wiley.com/doi/full/10.1002/ccd.28724
Abbreviations
Abbreviations | Full names |
AHA | American Heart Association |
ARTS | Arterial Revascularization Therapies Study |
ATO | Acute total occlusion |
CatLet | Coronary Artery Tree description and Lesion EvaluaTion |
CC | Collateral connections |
CTO | Chronic total occlusion |
DLCA | Diagonal-left circumflex area |
DMB | Distant main branch |
DOMA | Diagonal-obtuse marginal area |
Dx | Diagonals |
LAD | Left anterior descending artery |
LADex | Left anterior descending artery excluding diagonals |
LAO | Left anterior oblique |
LAVS | Left atrio-ventricular sulcus |
LCX | Left circumflex artery |
LIMA | Left internal mammary artery |
LM | Left main |
MB | Main branch |
PDA | Posterior descending artery |
PLVs | Posterolateral vessels |
PMB | Proximal main branch |
RCA | Right coronary artery |
RIMA | Right internal mammary artery |
SB | Side branch |
SYNTAX | SYNergy between percutaneous intervention with TAXus drug-eluting stents and cardiac surgery |
TIMI | The thrombolysis in myocardial infarction |
Myocardial blood supply is proportional to myocardial mass
Numerous studies have been performed to determine the actual flow to the left ventricular myocardium (1-8). These data demonstrate that actual myocardial blood is proportional to muscle mass (1,2,4-8). In other words, muscle mass can be utilized to estimate regional flow, and the importance of the blood vessels supplying this portion of myocardium.
Left ventricular segmentation
Because the 17 myocardial segment model is based on the approximately even division of the left ventricle as shown in Figure 1 (9), each segment can be understood either as 1 mass unit or as 1 actual flow unit. The importance of a blood vessel (weighting factor) depends on how many segments the blood vessel supplies rather than on the nomenclature of the blood vessel. The more segments a blood vessel supplies, the more important it is.

1. basal anterior | 7. mid anterior | 13. apical anterior |
2. basal anteroseptal | 8. mid anteroseptal | 14. apical septal |
3. basal inferoseptal | 9. mid inferoseptal | 15. apical inferior |
4. basal inferior | 10. mid inferior | 16. apical lateral |
5. basal inferolateral | 11. mid inferolateral | 17. apex |
6. basal anterolateral | 12. mid anterolateral |
Figure 1. Display, on a circumferential polar plot, of the 17 myocardial segments and the recommended nomenclature for tomographic imaging of the heart. Modified from reference (9).
Proposal of a benchmark type of coronary artery circulation among individuals
Although there is tremendous variability in the coronary artery blood supply to myocardial segments, it is generally considered appropriate to assign individual segments to specific coronary artery territories, which is defined as the benchmark type in this study (10). The assignment of the 17 segments to one of the 3 major coronary arteries is recommended by AHA Scientific Statement as shown in Figure 2 (9).

Figure 2. The 17 myocardial segments assigned to the territories of left anterior descending artery (LAD), right coronary artery (RCA), and left circumflex coronary artery (LCX). Reprinted from reference (9).
Division of the left heart into the three areas according to territories of coronary arteries in the benchmark type
In the benchmark type, the left heart is divided into 3 areas corresponding with the territories of the coronary arteries: the septal area with 6 segments, which are competitively perfused by LADex (LAD excluding diagonals) and PDA (posterior descending artery); the diagonal-obtuse marginal area (DOMA) with 8 segments, which are competitively perfused by diagonals and obtuse marginal arteries; and the inferior wall with 3 segments, which are competitively perfused by posterolateral vessels (PLVs) off RCA or LCX.
Competitive coronary blood supply accounts for tremendous variability in the coronary artery trees among individuals
The RCA and LCA provide competitive patterns of blood supply for the entire left heart and for the above described 3 areas. Specifically, LADex competes with PDA in supplying the septal area; diagonals compete with obtuse marginal branches in supplying the DOMA; and PLVs off RCA compete with PLVs off LCX in supplying the inferior wall. A pair of competitive blood vessels (RCA vs LCA, LADex vs PDA, etc.) conform to the law of growth and decline. That means a large RCA is associated with a small LCA, large diagonals with small obtuse marginal arteries, PLVs off RCA with small PLVs off LCX, long LAD with short PDA, and vice versa.
Reclassification of coronary artery circulation patterns
Reclassification of RCA dominance
The size of the RCA is defined depending on the distribution of the LCX according to the rule of competitive blood supply. Stem LCX usually courses in the atrio-ventricular sulcus and, on the way, gives rise to branches supplying the anterolateral wall, the inferolateral wall, and even the inferior wall in case of large LCX. At one extreme, a large LCX, with a diminutive RCA, provides blood flow to the anterolateral wall, inferolateral wall, the inferior wall and the inferior septum. At the other extreme, the LCX is small with perfusion of only a relatively small portion of the anterolateral wall, and the large RCA provides blood flow to the inferior septum, the inferior wall, the inferolateral wall and the remaining portion of the anterolateral wall.
Identification of the left atrio-ventricular sulcus (LAVS) on the angiograms in the left anterior oblique 40º/cranial 20º view (LAO 40º/cranial 20º view)
The stem LCX (not its branches) usually runs in the left atrio-ventricular sulcus (LAVS). Therefore, the stem LCX’s course on the angiograms can be utilized to indicate the LAVS. The crux cordis approximately falls upon the perpendicular line via the aorta ostium of the LCA (aorta wall) as shown on the angiograms. The crux cordis is the intersection point of the perpendicular line with the LAVS. In the LAO 40º/cranial 20º view, the LAVS runs from the upper right to the lower left, starting at the junction of the first quarter of the leftmost margin of the left heart with an approximately right angle referring to the left heart margin and terminating at the crux cordis.

Figure 3. Identification of the left atrio-ventricular sulcus (LAVS) on the angiograms in the LAO 40º/cranial 20º view. LCA angiography revealed LAD, LCX as well as RCA supply territories via the collateral connections in a RCA CTO patient.
Definitions of RCA sizes
In the LAO 40º/cranial 20º view, the LAVS is evenly divided into 3 parts from its starting point to the crux cordis.

Figure 4. Reclassification of RCA according to the LCX size in the LAO 40º/cranial 20º view.
PDA zero (left dominance): RCA gives no rise to any branches supplying the left ventricular myocardium. The entire left ventricular myocardium is supplied by the LCA. Figure 4a
PDA only: The stem LCX gives rise to a significant branch from the third part of the LAVS to supply the entire inferior wall in the LAO 40º/cranial 20º view. RCA provides blood flow only to the inferior septum. Figure 4b.
Small RCA: The stem LCX gives rise to a significant branch from the second part of the LAVS to supply a portion of the inferior wall in the LAO 40º/cranial 20º view. RCA provides blood flow to the inferior septum and the remaining portion of the inferior wall. Figure 4c.
Average RCA: The stem LCX gives rise to a significant branch from the first part of the LAVS to supply the inferolateral wall in the LAO 40º/cranial 20º view. RCA provides blood flow to the inferior septum and the entire inferior wall. Figure 4d.
Large RCA: The stem LCX gives no rise to a significant branch from the first part of the LAVS to supply the inferolateral wall, but only gives rise to branches to supply the anterolateral wall in the LAO 40º/cranial 20º view. RCA provides blood flow to the inferior septum, the inferior wall and the inferolateral wall. Figure 4e.
Super RCA: The stem LCX gives rise to small branches to supply a portion of the anterolateral wall in the LAO 40º/cranial 20º view. RCA provides blood flow to the inferior septum, the inferior wall, the inferolateral wall and the remaining portion of the anterolateral wall. Figure 4f.
Reclassification of diagonal size
The diagonal-obtuse marginal area (DOMA) of the left heart
The diagonal-obtuse marginal area (DOMA) of the left heart is competitively perfused by both diagonals (LAD) and obtuse marginal branches (LCX). In the LAO 40º / cranial 20º view, the DOMA takes on the approximate shape of a spindle delineated by discernable anatomical markers on angiographic coronary angiograms. Before giving rise to obtuse marginal arteries, initial stem LCX courses usually transversely in the atrioventricular sulcus and delineates the upper border of the DOMA. LAD almost constantly courses in the anterior interventricular sulcus and delineates the right border of the DOMA. The DOMA’s left and inferior margins are recognizable because of sufficient contrast between the heart margin and its surrounding tissues on angiograms. An imaginary line 1 starting from the apex divides the DOMA into 2 similar portions. Another imaginary line 2 perpendicular to the line 1 at its midpoint also divides the DOMA into 2 portions. Thus, we get 4 quadrants counterclockwise over the DOMA: I, II, III, and IV as shown in Figure 5.

Figure 5. The diagonal-obtuse marginal area (DOMA) delineated by anatomical markers and its four quadrants in diastole on coronary angiograms in the LAO 40º / cranial 20º view (left). Note that the DOMA’s left border is based on the margin of the left heart, rather than on the obtuse marginal branches, where tremendous variability has been frequently observed in terms of their origins and their running over the DOMA. Two imaginary lines divide the DOMA into 4 quadrants on the schematic diagram (right).
Definitions of diagonal (Dx) sizes
Small Dx: Dx distributing over ≤2 quadrants is defined as small and supplies less than 1/2 of the entire anterior wall with approximately 1.5 or less segments (Figure 6a).
Inter. Dx: Dx distributing over 3~4 quadrants is defined as intermediate and supplies more than 1/2 of the entire anterior wall with approximately 1.5~3 segments (Figure 6b).
Large Dx: Dx distributing over > 4 quadrants is defined as large and supplies the entire anterior wall as well as a portion of the anterolateral wall in excess of 3 segments (Figure 6c).
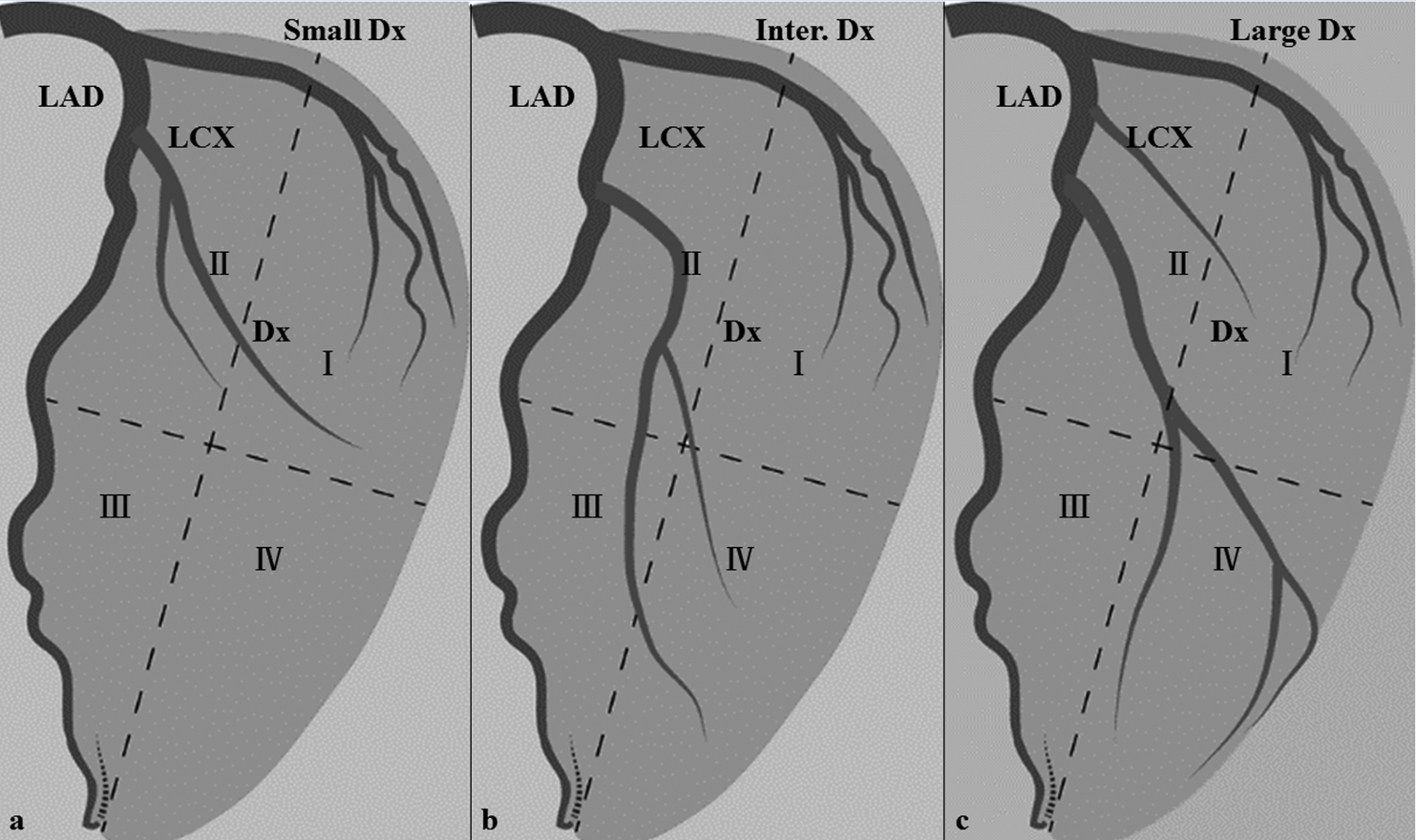 Figure 6. Reclassification of diagonal size according to its distribution over the four quadrants: Figures 6a indicated small diagonals; Figures 6b, intermediate diagonals; and Figure 6c, large diagonals.
Figure 6. Reclassification of diagonal size according to its distribution over the four quadrants: Figures 6a indicated small diagonals; Figures 6b, intermediate diagonals; and Figure 6c, large diagonals.
Reclassification of LAD length
Short LAD: LAD terminates before the apex and supplies the whole anterior septum with approximately 3 segments (Figure 7a);
Average LAD: LAD reaches the apex and supplies the whole anterior septum and the apex with approximately 4 segments with a terminal shape of inverted Y’ (Figure 7b);
Long LAD: LAD turns around the apex notch and runs further in the posterior interventricular sulcus, supplying the whole anterior septum, apex and a portion of posterior septum with approximately 5 segments (Figure 7c).

Figure 7. Different LAD lengths superimposed on the left heart surface in the vertical long axis view of the left heart at the level of anterior interventricular sulcus.
Reclassification by subdividing into 54 coronary circulation patterns
Six types of RCA dominance, 3 types of diagonal size, and 3 types of LAD length together result in a total of 54 patterns of coronary artery circulation, which are used to account for the tremendous variability in coronary anatomy among individuals.
评论列表: